International Journal of Virtual Worlds and Human Computer Interaction (VWHCI)
ISSN: 2368-6103

Volume 2, Year 2014 - Pages 37-46
DOI: 10.11159/vwhci.2014.005
Let's Kinect to Increase Balance and Coordination of Older People: Pilot Testing of a Balloon Catching Game
T. Claire Davies¹*, Thomas Vinumon¹, John Parsons², Lynne Taylor³
¹Department of Mechanical Engineering, University of Auckland,
Auckland, Private Bag 92019, New Zealand
c.davies@auckland.ac.nz
²School of Nursing, Faculty of Medical and Health Sciences, University of Auckland,
Auckland, Private Bag 92019, New Zealand
³School of Population Health, Faculty of Medical and Health Sciences,
University of Auckland, Auckland, Private Bag 92019, New Zealand
Abstract - The purpose of this research was to design, develop and assess the usability of an interactive rehabilitation game. User centered design in combination with serious gaming strategies were employed in the design of a targeted therapy programme to encourage at home balance retraining using specifically designed software with the Microsoft Kinect sensor. The development of this game involved a multi-disciplinary iterative design method employing the skills of physiotherapists, engineers and participants. Preliminary testing was conducted with younger adults and more formal testing with older participants to evaluate usability. Integrating the knowledge of all stakeholders increased the acceptability of the game by older participants. All were confident in the use of the technology and keen to increase their participation. Participants indicated on a usability questionnaire that these games are more engaging than typical therapy exercises. The games can be performed at home without the requirement for a partner and the participant can increase the game complexity depending on personal needs and preference. The time that the individual spends participating in the program and the results over several sessions can also be observed by the therapist allowing a better indication of adherence to therapy than self-report.
Keywords: Kinect, older people, physiotherapy, balance, coordination.
© Copyright 2014 Authors - This is an Open Access article published under the Creative Commons Attribution License terms. Unrestricted use, distribution, and reproduction in any medium are permitted, provided the original work is properly cited.
Date Received: 2013-09-15
Date Accepted: 2014-02-10
Date Published: 2014-03-31
1. Introduction
A serious concern, particularly of developed countries, is that an increase in the older population will undermine the sustainability of the public healthcare system. This is supported by data showing that per capita health expenditures are five times higher for people older than 75 years of age than for those aged 25–34 years [1]. One reason for high medical treatment costs among older people is an increased prevalence of chronic disease in older people associated with decreased mobility. These mobility impairments increase the risk of disability, falls, loss of independence and all-cause mortality in older people [2-4]. Yet, physical activity and exercise have the potential to slow the development of disability resulting from poor physical function [5]. Traditional exercise programs have proven to be effective at reducing the number of falls [6-8] and improving measures of function and mobility in older people, including those with neurological disorders, such as stroke [3, 9, 10]. Principles of exercise therapy that have been proven beneficial for enhancing coordination and balance are the use of bilateral synchronous activities [11, 12], repetition and task-orientated practice [10], all components that are readily incorporated into virtual reality gaming activities. The purpose of this research was to design, develop and assess the usability of an interactive game requiring the user to shift the upper body outside the base of support from one side to the other in a manner that was controlled and repeatable. We used a game based approach as gameification has been known to increase engagement, allows for collection of quantifiable data throughout the therapy program (at every session and among sessions), and has the ability to provide increased difficulty as the user becomes more proficient at each level.
2. Related Work
While traditional methods of therapy have been shown to be effective to increase balance for older people, there is often a lack of adherence in home-based exercises [13-15]. In an attempt to reduce the load on the therapist and provide a more cost-effective means of therapy, technologies have been introduced including robotics [16-18] and virtual reality [17, 19-21]. Rather than undergoing robotic therapies in a clinic environment, there has also been promise in the areas of gaming and virtual reality with readily available technologies like the Wii [21-24], the Sony EyeToy [19, 25-27] and more recently the Xbox Kinect [28]. Virtual reality gaming using off-the-shelf systems has been shown to improve measures of upper limb function in stroke survivors [29, 30] and balance in older people in community and hospital settings [31-34]. While these devices have been shown to be safe and feasible for home-based therapy treatment, off-the-shelf systems may not provide enough flexibility to allow a therapist to modify the exercise programme if the participant finds the exercises too difficult or gains enough confidence to attempt more challenging exercises. Other authors have noted that the speed of off-the shelf games is often too quick for the older person [35-37]. In addition, the feedback provided may not be sufficient to engage the user effectively [17, 38, 39] as the games often provide a score for a specific game rather than comparative scores over a given timeframe which shows improvement.
The benefits of these technologies are that they are inexpensive and can be easily implemented in the home environment, negating the need for therapist supervision. Perhaps their greatest benefit is that they provide real time feedback to the player and if designed effectively, are more enjoyable than traditional exercise, which may increase adherence.
To increase the acceptability of virtual reality gaming by older individuals, we used an iterative design approach engaging the users in the development of the system.
3. Methods
3.1. User Centered Game Design
User centered design requires a cyclic methodology and is governed by the International Standards Organisation 9241-10:2010 Human Centered Design for Interactive Systems; a Standard of which very few engineers are aware or choose to ignore. The key criteria of this process include: explicitly understanding the needs of the users while engaging a multi-disciplinary design team, involving the users throughout the design process and driving design by user involvement and feedback with continuous iteration. We sought to use these requirements in the design of a game to engage the user to move outside the base of support (off-balance) to increase general stability of older people.
3.2. Game Design Strategies
Serious gaming is an area of virtual reality that includes games that can be used to achieve a specific outcome of which the primary focus is not play [40]. An interdisciplinary approach that integrates the knowledge of engineers with clinicians enabled the development of a virtual reality home-based exercise program with off-the-shelf equipment. A therapist can change the goals for the patient and observe the patient's adherence from the data recorded. Our goal was the development of a serious game to encourage the participant to reach and step outside their base of support while focusing on another task.
3.3. Assessing Therapy Requirements: Stakeholder Input
Balloon volleyball is a common strategy for training balance. It is used as a method to challenge a person's standing balance with a degree of perturbations that are unpredictable. Ankle, knee, hip and stepping balance control strategies [41-44] are often employed as the balance challenge component of the task increases. In addition rehabilitation requires consideration of the principles of motor learning [45-49] in order to produce optimal outcomes. These include: the benefits of functional and meaningful activities on the retention of skill;[50-52] the use of functional tasks [50-52]; the need for task specificity where the rehabilitation components focus on the desired outcome (in this case being able to maintain balance in standing and respond to perturbations of balance); and the need for high levels of repetition and balance [53, 54]. Balloon volleyball aligns to these key principles. However, the activity requires at least two people to pass the balloon to each other. We chose to develop a game that would allow keen balloon volleyball players the opportunity to practice independently at home while also being able to quantify functional improvement while stretching and reaching. The purpose of this clinical task was to require individuals to focus on catching a balloon. The activity was designed to employ stepping balance control strategies where the participant was required to move outside their base of support, as well to incorporate bilateral synchronous upper limb strategies to catch the balloon.
3.4. Serious Gaming Requirements
Rego et al. [55] have proposed a serious gaming taxonomy for rehabilitation. Using this taxonomy, the serious game for balance rehabilitation developed with the Kinect system was as follows:
- Application area: Falls prevention was the main area of research, hence training of coordination and balance. The game design required the individual to move outside the base of support to require stepping while focusing on another task (catching a balloon) with the use of both hands.
- Interaction technology: A virtual reality type interface with the user interacting with objects on a screen using the Microsoft Kinect sensor.
- Game interface: Two dimensional with the game being projected on a large projection screen or wide screen television.
- Number of players: Since this game was to be used for individual practice training, only one player at a time would need to play the game.
- Game Genre: The simulation of a balloon falling and the individual attempting to catch using both hands (it was determined that single hand capture did not require as much movement outside the base of support).
- Adaptability: This is needed to increase motivation and confidence. As the participant acquires basic skills, the level of difficulty needed to perform the task should be increased. It is important to ensure that the speed and drop location of the balloons is randomly distributed to prevent anticipatory actions.
- Progress monitoring: A therapist must be able to evaluate the participant's progress and increase the game complexity as the participant becomes more adept at the task. The sessions must be recorded to allow for an evaluation of weakness (for example, if an individual has difficulty stepping in one direction).
- Performance feedback: Measureable rapid feedback was necessary to create the required motivation for the patients and to measure the performance of the patients after each session of practice.
- Portability: As the system requires only the Kinect sensor and a computer, the system is easily portable to a participant's house.
In addition to the requirements for serious gaming, other important criteria included:
- Simplicity - This being an unproven technology for rehabilitation programmes, initial feedback required of the system was to be assessed. The patient's involvement and motivation also needed to be considered. A complex, high speed game could generate frustration among the patients affecting the feedback and outcomes.
- Visually appealing - Playing a game in a rehabilitation programme with a dull environment generates less interest when compared to the multi coloured environment with other attractive features like dynamic change of colours, etc.
- Movement and appearance of virtual objects – It is more challenging to chase moving objects. This is an inherent characteristic of humans which is commonly seen among children. The same can be applied to patients during the initial phase of rehabilitation.
- Challenging - For the player, every game has to push the patients to the edge where they have to stretch slightly beyond their perceived limits. This is the most essential feature to make the patient acquire the skill.
3.5. Hardware
The Kinect sensor with the downloadable software development kit (SDK) was used to develop the game. The technology enables the Kinect to "perceive" the environment in front of the sensors in 3D form and then translates these perceptions into a synchronized depth image. The Kinect has a depth sensor, a RGB camera and a CPU inside. The CPU acquires the depth image by directing the infrared light at the person. The image sensor then reads the coded reflected light back from the person/scene. The device then processes the data to create an accurate per-frame depth image. All sensory information like depth image, colour image and audio is then transferred to the console connected to the Kinect [56]. The Microsoft software is used to match the person's avatar with the images sensed by the camera.
3.6. Participant Testing
Ethics approval was obtained from the University of Auckland Human Participant Ethics Committee to use this testing protocol for evaluation of the therapeutic game. Two different testing stages were conducted to allow for iterative improvement throughout the design process.
3.6.1. Preliminary Testing with Younger Adults
The game was evaluated by five typically developed adults to evaluate reaction time and movements. Each participant completed each of the three levels (slow, medium and fast), then completed a questionnaire developed by Lange et al. (2010) focussing on game enjoyment, level of exertion, ease of use and general satisfaction with the game [57].
The younger adults who participated were generally familiar with computers and gaming. Two had seen rehabilitation programs, but not virtual reality gaming techniques for rehabilitation. During the gaming trials, observations were recorded by the researchers. Although all participants reported that the game was easy, no individual achieved a perfect score during testing.
3.6.2. Game Changes after Initial Resting
Upon receiving general comments from the testing by both younger participants and two physiotherapists who observed the testing procedure, the following changes were made to the interface.
1. The font size of the display was increased to allow older participants to effectively read their scores.
2. A confined area of interaction space was defined. Loss of sensor detection occurs when beyond sensor range from which it is hard to recover.
3. Further investigation was required into the Kinect function to reduce the time lag between movements of the individual and the avatar response. This issue does appear to be inherent within the system (http://www.1up.com/news/kinect-lag-eliminated-developer). Responding to this time lag requires practice by the user, but the player should be able to feel the time lag and react accordingly. This is similar to the actions required in vehicle response when driving (a time lapse occurs between action of the driver and reaction of the vehicle).
After incorporating changes to the software from the group of younger adults, the following game resulted.
3.7. Description of the Game
Balloons of different colour drop from the top of the screen and the participant must catch the balloon with both hands. The player's hand positions are projected on the screen to allow a visual interception of the hand with the balloon. The balloon drops straight down along any of eight lines across the screen from random locations. The participant has to move his body (not just his upper extremity) to capture the balloons to the extreme right and left sides. This requires the participant to shift the centre of weight while focusing on hand manipulation rather than concentrating on foot placement. The screen was divided into quadrants; upper and lower for each side. The scores were distributed across the quadrants such that if the balloon was caught in the upper quadrants (faster reaction time), the score was twice that in the lower quadrant. The speed of the falling object or balloon could be controlled by entering the time interval in the program (or the slow, medium or fast selection on the first screen of the program – equivalent to 8/min, 15/min, or 30/min respectively if none were caught). Catching the balloons meant that more dropped in the same timeframe. The goal of the game is to collect as many balloons as possible in a given time period (for our study this was set at 1 minute for medium and fast speeds and 2 minutes for the slow speed).
3.8. Data Analysis
On completing the game, the number of balloons successfully caught towards the right, centre and left of the screen were displayed. Although initial performance characteristics were only displayed as a score, the final design included a percentage average score calculated as follows:
|
|

as well as a message. Three cut-off percent values were decided and their corresponding messages-
For % Avg. value ≤ 50% the message was – "GOOD JOB. BETTER LUCK NEXT TIME".
For 50% < % Avg. value ≤ 75% the message was – "YOU CAN DO BETTER"
For 75% < % Avg. value ≤ 100% the message was – "EXCELLENT JOB".
In addition, performance evaluation graphs for each game were displayed. The graphical representation gives feedback to the user in an efficient manner. The scores of each game are stored in XML format for last 5 games played.
The responses for the Likert scales from the usability questionnaires were analysed using chi-squared test to determine if there was a difference between the older group and the younger participants. The comments made by participants were analysed using a general inductive approach as this is a commonly used systematic procedure used for analysing qualitative data [58].
3.9. Formal Testing with Older Participants
Five older participants (greater than 75 years) were invited for the trial. Each participant was briefed on the trial procedure and was given some practice time to better understand how to manipulate the "hands" on the screen. Each participant filled out a usability questionnaire (from Lange et al. [57]) that included a Likert based scale from 1 to 5 to answer each question. The participant demographics can be found in Table 1.
Table 1. Demographics of Older Participants.
|
Participant |
Age/Gender |
Participant Characteristics |
Observations |
|
1 |
82 F |
Independent Good cognition Slow gait Slow upper limb movement Hand tremor |
Difficulty detecting hand movement by sensor Took several steps in the direction of the dropping balloon leaving insufficient time to return before next drop. Unsuccessful trial |
|
2 |
78 F |
Independent Slow gait |
Initially successful Loss of sensor detection when participant moved beyond range of sensor for a second |
|
3 |
79 M |
Independent Slow gait |
Successful at "slow" drops Good anticipation and reaction Difficulty at right and left extremes, especially if one balloon dropped at right, followed by one at the left. |
|
4 |
77 M |
Independent Parkinson's disease |
Very successful at all three levels |
|
5 |
88 F |
Independent Walking stick Slight tremors |
Very successful at all three levels |
4. Results
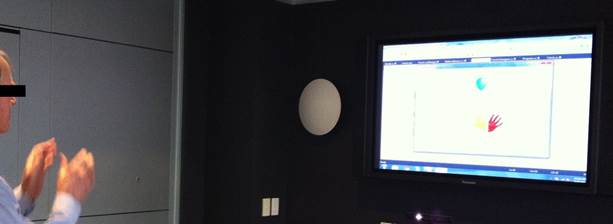
Participants were generally quite pleased with the game and became engaged (Figure 1 and observations by the researchers during the testing documented in Table 1). Figure 1 shows an individual engaged in the game. Note the balloons falling from the top of the screen, while the hands attempt to grasp it.
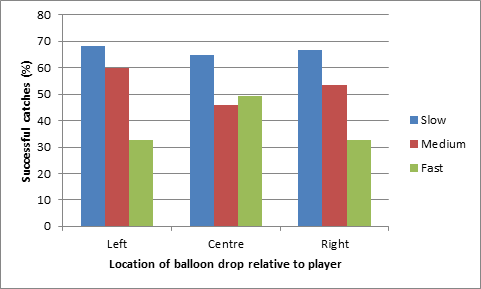
4.1. Quantitative Measures of Success
The % success rate at each of the speeds and at each of the locations can be observed in Figure 2 (Participants 1 and 2 did not complete the medium and fast speeds). Although the first two participants appeared to have difficulties, three were very successful. For the balloons dropping in the centre of the screen, the participant did not move outside the base of support and was generally quite stable. When the participant was required to reach to the right or to the left, the game became more difficult and the participant's balance was challenged as they reached from one side to the other.
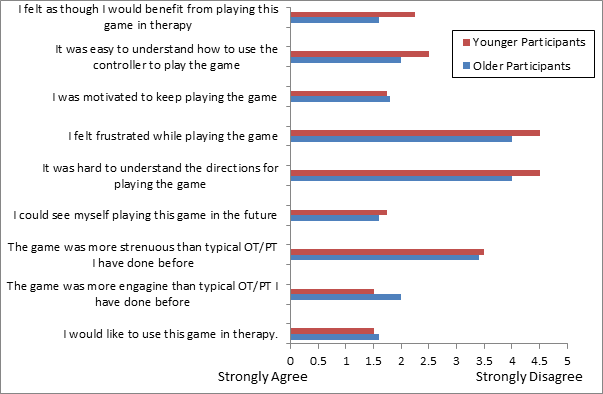
4.2. Usability Questionnaire Feedback from All Participants
Each of the participants (from both the preliminary trial and the formal trial) was asked to answer a questionnaire to collect general feedback on the programme [57]. The results from the questionnaire are listed in Figure 3. There were no significant differences between younger and older participants for any of the questions except for the question "I feel as though I would benefit from playing with this game in therapy". Older adults judged the game as being significantly more beneficial for therapy than younger participants (younger = 2.75 and older = 3.5, p=0.054).
4.3. Qualitative Responses
Participants were permitted to add comments to their evaluations. In general, the participants liked the game and commented that it was similar to the real balloons they have used in training. They found the use of the Kinect innovative and interesting and were surprised to see it adapted to a rehabilitation programme for their benefit. There was mixed response about the challenge involved, though the three different levels presented adequate challenge overall. A wide screen TV was used in the testing, but many commented that they do not have access to a large screen at home and may be difficult to implement in a home environment. Most importantly, loss of detection of the hands of participants can be a very de-motivating factor. Another option to increase motivation may be to add auditory feedback.
5. Discussion
This paper discusses an iterative approach to the development of a game for individuals with balance impairments. The most important aspect of designing such a game is the interaction with the users throughout the process. Many games are developed prior to effective testing and this limits their usefulness. Principles of motor learning and exercise therapy were important in the game design. Exercise programs have shown that coordination and balance is enhanced with bilateral synchronous activities [11, 12], which was achieved by the requirement to coordinate two hands while catching the balloon, and repetition [10], achieved by multiple balloons dropping at varying locations at each given level. In our case, we tested control participants to ensure that the system was effective, and proceeded to test participants who were within the population to which we wanted to appeal. By integrating the requirements of game design for serious gaming with feedback from younger participants, older participants, and therapists, a system was developed that could effectively meet the needs of both the therapists and the participants.
Although young adult participants all commented that the game was easy, none achieved a perfect score. This suggests that the game is challenging enough to allow for increasing difficulty across therapy sessions. The same was observed for the at home trial conducted as the participant continued to play the "fast version" of the game, while still not achieving a perfect score. It will now be important to evaluate the therapy treatment as compared to traditional methods of treatment to evaluate the effectiveness of this gaming protocol.
The results from the usability questionnaire showed that in general, the participants all found the game motivating, beneficial for therapy and easy to control. Of note, the individual who participated in the game for an at-home trial gave full marks for these questions, an improvement on his initial rating. Few negative responses were reported, though this may be due to the novelty of the equipment, game and task. The older adults appeared to find the game more frustrating and harder to use, but this was not significant. They did however indicate that they can see the game being more beneficial to therapy than the younger population. The younger population doesn't have a need to undergo balance therapy and thus wouldn't judge this question of importance.
Although gaming has been used for participants with stroke using off the shelf technology, only a limited number of Kinect games that are specific for older adults have been developed for upper limb rehabilitation. Those that have been developed only require the individual to move to a stationary object and use one hand [59, 60], while the game discussed herein used a bimanual grasping task that more closely simulated clinic rehabilitation.
Positive responses were observed throughout the iteration process from all users, but it is not possible to predict whether increased adherence will result when using the system as compared to traditional means of therapy. Further studies are needed to evaluate adherence, increased balance control and continued enjoyment of the therapy.
6. Conclusions
User Centred Design methods in the development of a game are important to ensuring satisfaction with the game from the perspective of clinicians and participants. The Kinect was effectively used in the process of designing and developing an interactive game that required the user to shift the upper body outside the base of support from one side to the other in a manner that was controlled and repeatable. The users commented that the game was more engaging than typical physiotherapy sessions. This game wascreated for the purpose of rehabilitation and enabled effective interaction with the gaming environment while attempting to improve balance strategies. Further testing is required to evaluate effectiveness of this therapy over time, but this study showed that the multidisciplinary approach was effective in providing users with an engaging interactive game.
References
[1] U. Reinhardt, "Does the aging of the population really drive the demand for health care?" Health Affairs, 22(6), 2003 p. 27-39. View Article
[2] M. Hirvensalo, T. Rantanen, and E. Heikkinen, "Mobility difficulties and physical activity as predictors of mortality and loss of independence in the community-living older population" Journal of the American Geriatrics Society, 48(5), 2000, p. 493.View Article
[3] M.A.F. Singh, "Exercise comes of age, rationale and recommendations for a geriatric exercise prescription" Journals of Gerontology Series A, Biological Sciences & Medical Sciences, 57A(5), 2002, p. M262-82.View Article
[4] N. Lundebjerg, "Guideline for the prevention of falls in older persons" Journal of the American Geriatrics Society, 49(5), 2001, p. 664-672. View Article
[5]T.M. Gill, D. I. Baker, M. Gottschalk, P.N. Peduzzi, H. Allore and A. Byers "A program to prevent functional decline in physically frail, elderly persons who live at home" New England Journal of Medicine, 347(14), 2002, p. 1068-74. View Article
[6] D.M. Buchner, M.E. Cress, B.J. de Lateur, P.C. Esselman, A.J. Margherita, R. Price, E.H. Wagner "The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults" Journals of Gerontology Series A-Biological Sciences & Medical Sciences, 52(4), 1997, p. M218-24. View Article
[7] M.M.R. Gardner, M.C. McGee, & A.J. Campbell, "Application of a falls prevention program for older people to primary health care practice" Preventive Medicine, 34(5), 2002, p. 546-553. View Article
[8] S.R. Lord, S. Castell, J. Corcoran, J. Dayhew, B. Matters, A. Shan, P. Williams "The effect of group exercise on physical functioning and falls in frail older people living in retirement villages, a randomized, controlled trial" Journal of the American Geriatrics Society, 51(12), 2003, p. 1685-92. View Article
[9] A.D. Beswick, K. Rees, P. Dieppe, S. Ayis, R. Gooberman-Hill, J. Horwood, S. Ebrahim "Complex interventions to improve physical function and maintain independent living in elderly people, a systematic review and meta-analysis" Lancet, 371(9614), 2008, p. 725-735. View Article
[10] P. Langhorne, F. Coupar, and A. Pollock, "Motor recovery after stroke, a systematic review" The Lancet Neurology, 8(8), 2009, p. 741-754. View Article
[11] J.J. Summers, F.A. Kagerer, M.I. Garry, C.Y. Hiraga, A. Loftus, J.H. Cauraugh "Bilateral and unilateral movement training on upper limb function in chronic stroke patients, A TMS study" Journal of the Neurological Sciences, 252(1), 2007, p. 76-82. View Article
[12] J.H. Cauraugh and J.J. Summers, "Neural plasticity and bilateral movements, A rehabilitation approach for chronic stroke" Progress in Neurobiology, 75(5), 2005, p. 309-320. View Article
[13] K.K. Miller, "Adherence with home exercise programs 1-6 months after discharge from physical therapy by individuals post-stroke" in School of Health and Rehabilitation Sciences, Indiana University, 2011,p. 56. View Article
[14] J.H. Rimmer, E. Wang, and D. Smith, "Barriers associated with exercise and community access for individuals with stroke" Journal of Rehabilitation Research and Development, 2008. 45(2), p. 315-22. View Article
[15] J.S. Schneider, "Evaluating exercise adherence, a solution focused approach" in Psychology, California State University, Chico, 2011, p. 55. View Article
[16] A.C. Lo, P.D. Guarino, L.G. Richards, J.K. Haselkorn, G.F. Wittenberg, D.G. Federman, R.J. Ringer, T.H. Wagner, H.I. Krebs, B.T. Volpe, C.T. Bever, D.M. Bravata, P.W. Duncan, B.H. Corb, A.D. Maffucci, S.E. Nadeau, S.S. Conroy, J.M. Powell, G.D. Huang, P. Peduzzi "Robot-Assisted Therapy for Long-Term Upper-Limb Impairment after Stroke" New England Journal of Medicine, 362(19), 2010, p. 1772-1783. View Article
[17] S. Brochard, J. Robertson, B. Médée, O. Rémy-Néris "What's new in new technologies for upper extremity rehabilitation?" Current Opinion in Neurology. 23(6), 2010, p. 683-687. View Article
[18] O. Peter, G. Fazekas, J. Zsiga, Z. Dénes "Robot-mediated upper limb physiotherapy, review and recommendations for future clinical trials" International Journal of Rehabilitation Research, 34(3), 2011, p. 196-202. View Article
[19] S. Flynn, P. Palma, and A. Bender, "Feasibility of using the Sony PlayStation 2 gaming platform for an individual poststroke, a case report" Journal of Neurologic Physical Therapy, 31(4), 2007, p. 180-9. View Article
[20] A. Henderson, N. Korner-Bitensky, and M. Levin, "Virtual Reality in Stroke Rehabilitation, A Systematic Review of its Effectiveness for Upper Limb Motor Recovery" Topics in Stroke Rehabilitation, 14(2), 2007, p. 52-61. View Article
[21] M.R. Mouawad, C.G. Doust, P.A. McNulty "Wii-based movement therapy to promote improved upper extremity function post-stroke, a pilot study" Journal of Rehabilitation Medicine, 43(6), 2011, p. 527-33. View Article
[22] G. Saposnik, R. Teasell, M. Mamdani, W. McIlroy, D. Cheung, K.E. Thorpe, L.G. Cohen, M. Bayley "Effectiveness of Virtual Reality Using Wii Gaming Technology in Stroke Rehabilitation" Stroke. 41(7), 2010, p. 1477-1484. View Article
[23] J.K. Hsu, R. Thibodeau, S.J. Wong, D. Zukiwsky, S. Cecile, D.M. Walton "A "Wii" bit of fun, the effects of adding Nintendo Wii((R)) Bowling to a standard exercise regimen for residents of long-term care with upper extremity dysfunction" Physiotherapy Theory and Practice, 27(3), 2011, p. 185-93. View Article
[24] L. Yong Joo, Y.T. Soon, D. Xu, E. Thia, F.C. Pei, C.W. Kuah, K.H. Kong "A feasibility study using interactive commercial off-the-shelf computer gaming in upper limb rehabilitation in patients after stroke" Journal of Rehabilitation Medicine. 42(5), p. 437-41. View Article
[25] G. Yavuzer, A. Senel, M.B. Atay, H.J. Stam "''Playstation eyetoy games'' improve upper extremity-related motor functioning in subacute stroke, a randomized controlled clinical trial" European Journal of Physical and Rehabilitation Medicine, 44(3), 2008, p. 237-44. View Article
[26] M. Sandlund, E.L. Waterworth, and C. Hager, "Using motion interactive games to promote physical activity and enhance motor performance in children with cerebral palsy" Developmental Neurorehabilitation, 14(1), 2011, p. 15-21. View Article
[27] D. Rand, R. Kizony, and P.T. Weiss, "The Sony PlayStation II EyeToy, low-cost virtual reality for use in rehabilitation" Journal of Neurological Physical Therapy, 32(4), 2008, p. 155-63. View Article
[28] L.M. Taylor, R. Maddison, L.A. Pfaeffli, J.C. Rawstorn, N. Gant, N.M. Kerse "Activity and Energy Expenditure in Older People Playing Active Video Games" Archives of Physical Medicine and Rehabilitation, 93(12), 2012, 2281-2286. View Article
[29] G. Saposnik, M. Levin, and f.t.S.O.R.C.W. Group, "Virtual Reality in Stroke Rehabilitation, A Meta-Analysis and Implications for Clinicians" Stroke, 42(5), 2011, p. 1380-1386.View Article
[30] K. Laver, S. George, S. Thomas, J.E. Deutsch, M. Crotty "Cochrane review, Virtual reality for stroke rehabilitation" European Journal of Physical and Rehabilitation Medicine, 48(3), 2012, p. 523-530. View Article
[31] A.A. Rendon, E.B. Lohman, D. Thorpe, E.G. Johnson, E. Medina, B. Bradley "The effect of virtual reality gaming on dynamic balance in older adults" Age and Ageing, 41(4), 2012, p. 549-552. View Article
[32] D. Schoene, S.R. Lord, K. Delbaere, C. Severino, T.A. Davies, S.T. Smith "A Randomized Controlled Pilot Study of Home-Based Step Training in Older People Using Videogame Technology" Plos One, 8(3), 2013. View Article
[33] C-H. Lai, C-W. Peng, Y-L Chen, C-P. Huang, Y-L. Hsiao, S-C. Chen "Effects of interactive video-game based system exercise on the balance of the elderly" Gait and Posture, 37(4), 2013, p. 511-515. View Article
[34] K. Laver, S. George, J. Ratcliffe, S. Quinn, C. Whitehead, O. Davies, M. Crotty "Use of an interactive video gaming program compared with conventional physiotherapy for hospitalised older adults, A feasibility trial" Disability and Rehabilitation, 34(21), 2012, p. 1802-1808. View Article
[35] H.C. Higgins, J.K. Horton, B.C. Hodgkinson, S.B. Muggleton "Lessons learned, Staff perceptions of the Nintendo Wii as a health promotion tool within an aged-care and disability service" Health Promotion Journal of Australia, 21(3), 2010, p. 189-195. View Article
[36] D. Harley, G. Fitzpatrick, L. Axelrod, G. White, G. McAllister "Making the Wii at home, Game play by older people in sheltered housing" Lecture Notes in Computer Science, 6389, 2010 p. 156-176. View Article
[37] E. Cyarto, S. Kuys, T. Henwood, I. Blackberry "Can Wii™ work it out?" Telecommunications Journal of Australia, 61(3), 2011. View Article
[38] K.M. Gerling, J. Schild, and M. Masuch, "Exergame design for elderly users, the case study of SilverBalance" in Proceedings of the 7th International Conference on Advances in Computer Entertainment Technology, ACM, Taipei, Taiwan, 2010, p. 66-69. View Article
[39] N. Mumford and P.H. Wilson, "Virtual reality in acquired brain injury upper limb rehabilitation, Evidence-based evaluation of clinical research" Brain Injury, 23(3), 2009, p. 179-191. View Article
[40] D.R Michael, S.L. Chen "Serious games, Games that educate, train, and inform" 2005, Muska & Lipman/Premier-Trade.
[41] L.A. Brown, A. Shumway-Cook, & M.H. Woolacott, "Attentional demands and postural recovery, the effects of ageing" The Journals of Gerontology, 54A(4), 1999, p. M165-M171. View Article
[42] S.I. Lin, & M.H. Woolacott, "Postural muscle responses following changing balance threats in young stable older and unstable older adults" Journal of Motor Behaviour, 34(1), 2002, p. 37-47. View Article
[43] D. Manchester, M.H. Woolacott, N. Zederbauer, & O. Marin, "Visual, vestibular and somatosensory contributions to balance control" Journal of Gerontology, 44, 1898, p. M118-M127. View Article
[44] M. Woolacott, A. Shumway-Cook & L.M. Nasner, "Aging and posture control, changes in sensory organisation and muscular coordination" International Journal of Aging and Human Development, 23, 1986, p. 97-114. View Article
[45] A.M. Haith and J.W. Krakauer, "Theoretical models of motor control and motor learning" Routledge handbook of motor control and motor learning, 2013, p. 7. View Article
[46] J. Izawa, T. Rane, O. Donchin, R. Shadmehr "Motor adaptation as a process of reoptimization" The Journal of Neuroscience, 28(11), 2008, p. 2883-2891. View Article
[47] J.W. Krakauer and P. Mazzoni, "Human sensorimotor learning, adaptation, skill, and beyond" Current Opinion in Neurobiology, 21(4), 2011, p. 636-644. View Article
[48] J.E. Schlerf and R.B. Ivry, "Task goals influence online corrections and adaptation of reaching movements" Journal of Neurophysiology, 106(5), 2011, p. 2622-2631. View Article
[49] R.A. Schmidt, "Motor learning & performance" From principles to practice. 1991, Human Kinetics Books.
[50] M.N. Holubar and M.S. Rice, "The effects of contextual relevance and ownership on a reaching and placing task" Australian Occupational Therapy Journal, 53(1), 2006, p. 35-42. View Article
[51] K.-c. Lin, C.Y. Wu, C.L. Chenm J.S. Chern, W.H. Hong "Effects of object use on reaching and postural balance, a comparison of patients with unilateral stroke and healthy controls" American journal of Physical Medicine & Rehabilitation, 86(10), 2007, p. 791-799. View Article
[52] S. Hetu and C. Mercier, "Using purposeful tasks to improve motor performance, does object affordance matter?" The British Journal of Occupational Therapy, 75(8), 2012, p. 367-376. View Article
[53] L. Richards and P. Pohl, "Therapeutic interventions to improve upper extremity recovery and function" Clinics in geriatric medicine, 15(4), 1999. View Article
[54] C.E. Lang, J.R. MacDonald, and C. Gnip, "Counting repetitions, an observational study of outpatient therapy for people with hemiparesis post-stroke" Journal of Neurologic Physical Therapy, 31(1), 2007, p. 3-10. View Article
[55] P. Rego, P.M. Moreira, and L.P. Reis. "Serious games for rehabilitation, A survey and a classification towards a taxonomy" in 5th Iberian Conference on Information Systems and Technologies (CISTI), 2010. View Article
[56] J. Weidi, Y.Won-Jae, J. Saniie, E. Oruklu "3D image reconstruction and human body tracking using stereo vision and Kinect technology" In Electro/Information Technology (EIT), 2012 IEEE International Conference on. 2012. View Article
[57] B. Lange, S. Flynn, R. Proffitt, C.Y. Chang, A.S. Rizzo "Development of an interactive game-based rehabilitation tool for dynamic balance training" Top Stroke Rehabilitation, 17(5), 2010, p. 345-52. View Article
[58] D.R. Thomas, "A General Inductive Approach for Analyzing Qualitative Evaluation Data" American Journal of Evaluation, 27(1), 2006, p. 1-10. View Article
[59] B. Lange, S. Koening, E. McConnell, C. Chang, R. Juang, E. Suma, M. Bolas, A. Rizzo "Interactive game-based rehabilitation using the Microsoft Kinect" in 19th IEEE Virtual Reality Conference, VR 2012, March 4, 2012 - March 8, 2012. 2012. Costa Mesa, CA, United states, IEEE Computer Society. View Article
[60] M.-C. Huang, E. Chen, W. Xu, M. Sarrafzadeh "SmartGlove for upper extremities rehabilitative gaming assessment" In 5th International Conference on Pervasive Technologies Related to Assistive Environments, PETRA 2012, June 6, 2012 - June 8, 2012. 2012. Heraklion, Crete, Greece, Association for Computing Machinery. View Article